Nobody looks forward to getting a Pap test, but we women get them regularly – or SHOULD get them regularly because Pap tests are crucial to preventing cervical cancer. We at Cervivor want to make sure that women understand what a Pap test does, what it is looking for and what “abnormal” results may mean. Afterall, if your Pap results came back abnormal, it is important to understand what that means and what steps to take next.
What exactly is a Pap test?
A Pap test looks for abnormalities and precancerous cell changes in the cervix. If not treated, these abnormal cells could lead to cervical cancer.
Each year, more than 50 million Pap tests are performed in the U.S. to screen for cervical cancer. An estimated 3 million of these Pap tests (5%) are read as abnormal. In fact, approximately 20% of American women have had at least one abnormal Pap test result in their lifetimes, though in the majority of cases, the abnormal cells are the result of a bacterial or yeast infection and are not pre-cancerous or cancerous. While less than 1% of abnormal Paps result in a cervical cancer diagnosis, up to 1 million Paps find early, potentially pre-cancerous cells that can be easily removed before they progress. This is why follow-up of abnormal Pap results is critical!
Pap test results will come back to your doctor as either:
- Normal. The cells collected from your cervix during the Pap test look like they should.
- Unclear. If results are unclear, your doctor may do more testing right away to rule out any problems, or your doctor may have you come back in 6 months or a year for another Pap test.
- Abnormal. The cells collected from your cervix during your Pap test look abnormal. The first thing to keep in mind: abnormal Pap test results do not mean you have precancer or cancer. Sometimes the changed cells are due bacteria or yeast. But important follow-up tests will need to be done to get more information.
What are some of the follow-ups for abnormal Pap test results?
You may need more tests to find out if you have an HPV infection and/or to find out how severe the cell changes are. For example, your doctor may do:
- An HPV test. Like a Pap test, an HPV test is done on a sample of cells taken from the cervix to see if the abnormalities were caused by infection with any of the types of human papillomavirus that are linked to cervical cancer.
- Another Pap test in about 6 to 12 months (“watchful waiting”).
- A colposcopy, a test to look at the vagina and cervix through a lighted magnifying tool.
What does a colposcopy look for?
A colposcopy is when a microscope (colposcope) with a strong light will be used to look at your cervix. Hundreds of thousands of colposcopies are performed in the U.S. each year. If any abnormal areas are identified, the doctor may take a small sample of tissue (“biopsy”) from the cervix for closer examination. A biopsy is similar to a small pinch in terms of sensation and shouldn’t be too painful. The purpose of a biopsy is to confirm whether your screening test has been correct in identifying a problem.
The colposcopist will usually be able to tell straight away if there are abnormal cells in your cervix, but biopsy results can take a few days to a few weeks to receive.
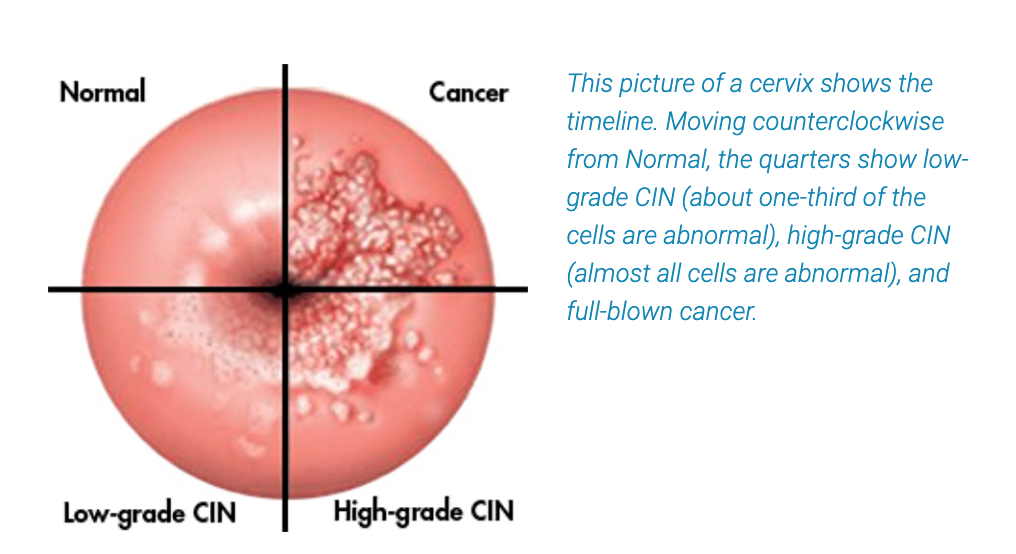
Understanding the Language Used to Describe Cervical Cell Abnormalities
Treatment, if any, will depend on whether your abnormal cell changes are mild, moderate, or severe. Pap and biopsy results reports commonly use these terms to report the severity of cell changes:
- Mild: ASC-US or ASC-H. These are changes for which the cause is unknown. ASC-US (atypical squamous cells of undetermined significance) changes usually stay the same or return to normal. ASC-H (ASC that cannot exclude high-grade squamous intraepithelial lesions) changes are also minor but have a higher likelihood of becoming more serious.
- Mild: LSIL (low-grade squamous intraepithelial lesions). These changes, also known as CIN 1 (cervical intraepithelial neoplasia) are mild but may be more likely to become more severe over time, though could return to normal.
- Moderate to Severe: HSIL and AGC: These moderate to severe cell changes require follow-up. HSIL (high-grade squamous intraepithelial lesions) and atypical glandular cells (AGC) may also be referred to as CIN II and CIN III are more likely to be precancerous and turn into cervical cancer if left untreated.
Treatments to remove abnormal, precancerous cells:
The good news is, abnormal or precancerous cells can be removed from your cervix. Your doctor will likely recommend one of the following procedures:
- LEEP (loop electrosurgical excision procedure): A thin, low-voltage electrified wire loop is sued to cut out abnormal cervical cells.
- Laser or “cold-knife” conization (also referred to as a cone biopsy): A laser or scalpel (“cold-knife”) removes a cone or cylinder-shaped piece of the cervix.
- Laser therapy: A tiny beam of high-intensity light vaporizes and destroys abnormal cells.
- Cryotherapy: A very cold probe freezes and destroys abnormal cells.
There is a wealth of information out there from the American College of Obstetricians & Gynecologists, from the Foundation for Women’s Cancer and of course, from Cervivor.
As a community of cervical cancer survivors, we encourage you to stay calm, ask questions, and be diligent about your follow-up testing.